Short dental implants were looked upon unfavorably until very recently. But gradually with newer designs, surfaces and better evidence it seems that this is gradually changing. In fact when I first began in implant dentistry 10mm was considered a short implant. Today anything shorter than 7 is a short implant. That's a significant change ! Some systems offer implants as short as 5mm albeit in wide diameters only. Ante's law and rules about Crown to Implant ratio seem not to apply in the same way to implants as to teeth. Advertisements for companies such as Bicon and Endopore regularly feature pictures of implant restorations that seem to defy every rule of conventional prosthodontics and still seem to thrive if the votaries of the system are to be believed !
Finally it is the gradual accretion of studies such as the one below that will convince us of the effectiveness of 'short implants' as an accepted modality of treatment.
Short Dental Implants
A Systematic Review
Abstract
Growing evidence has suggested the utility of short dental implants for oral reconstructive procedures in clinical situations of limited vertical bone height. The aim of this review was to systematically evaluate clinical studies of implants < 10 mm in length, to determine short implant-supported prosthesis success in the atrophic jaw. Implant survival, incidence of biological and biomechanical complications, and radiographic peri-implant marginal bone loss were evaluated. Screening of eligible studies, quality assessment, and data extraction were conducted by two reviewers independently. Meta-analyses were performed by the pooling of survival data by implant surface, surgical technique, implant location, type of edentulism, and prosthetic restoration. Two randomized controlled trials and 14 observational studies were selected and analyzed for data extraction. In total, 6193 short-implants were investigated from 3848 participants. The observational period was 3.2 ± 1.7 yrs (mean ± SD). The cumulative survival rate (CSR) was 99.1% (95%CI: 98.8-99.4). The biological success rate was 98.8% (95%CI: 97.8-99.8), and the biomechanical success rate was 99.9% (95%CI: 99.4-100.0). A higher CSR was reported for rough-surfaced implants. The provision of short implant–supported prostheses in patients with atrophic alveolar ridges appears to be a successful treatment option in the short term; however, more scientific evidence is needed for the long term.

 Orthopedic and maxillofacial surgeons sometimes prepare for surgery by creating physical models of 3D scans of bones that they need to work on. Such models are also useful in educating med school students, doctors, and patients. However, these models tend to be very expensive, usually seen only in well-funded research projects or used by expensive medical professionals. Oftentimes, because the cost of the model is so high, a compromise must be made, so the resulting models end up being truncated or less than actual size.
Orthopedic and maxillofacial surgeons sometimes prepare for surgery by creating physical models of 3D scans of bones that they need to work on. Such models are also useful in educating med school students, doctors, and patients. However, these models tend to be very expensive, usually seen only in well-funded research projects or used by expensive medical professionals. Oftentimes, because the cost of the model is so high, a compromise must be made, so the resulting models end up being truncated or less than actual size.
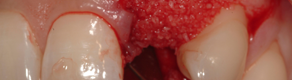
 Bone grafting is the use of either native, cadaveric, or artifical bone pieces to fill a void where you would like new bone to grow. Often at first, bone grafts have poor structural qualities and need hardware to protect them, the bone around and to keep them in place. In Oral-Maxillofacial surgery bone loss is often caused by infection, trauma, tumors and other conditions.
Bone grafting is the use of either native, cadaveric, or artifical bone pieces to fill a void where you would like new bone to grow. Often at first, bone grafts have poor structural qualities and need hardware to protect them, the bone around and to keep them in place. In Oral-Maxillofacial surgery bone loss is often caused by infection, trauma, tumors and other conditions.  Perhaps someday, the bi-annual trip to the dentist may become much less intimidating, thanks to researchers at Leeds University in the UK who have developed a completely pain-free way to fill cavities.
Perhaps someday, the bi-annual trip to the dentist may become much less intimidating, thanks to researchers at Leeds University in the UK who have developed a completely pain-free way to fill cavities. NovaBone Products has introduced a new line of biologically active bone-graft substitutes that are designed to enhance the body’s natural healing process by facilitating rapid vascularization and mineralization. Suspended in a rapidly-absorbable binder, the moldable material contains a calcium phosphosilicate with a continuous macroporous structure. Known as MacroPor-Si+, the product can be used to repair osseous defects throughout the skeletal system.
NovaBone Products has introduced a new line of biologically active bone-graft substitutes that are designed to enhance the body’s natural healing process by facilitating rapid vascularization and mineralization. Suspended in a rapidly-absorbable binder, the moldable material contains a calcium phosphosilicate with a continuous macroporous structure. Known as MacroPor-Si+, the product can be used to repair osseous defects throughout the skeletal system.